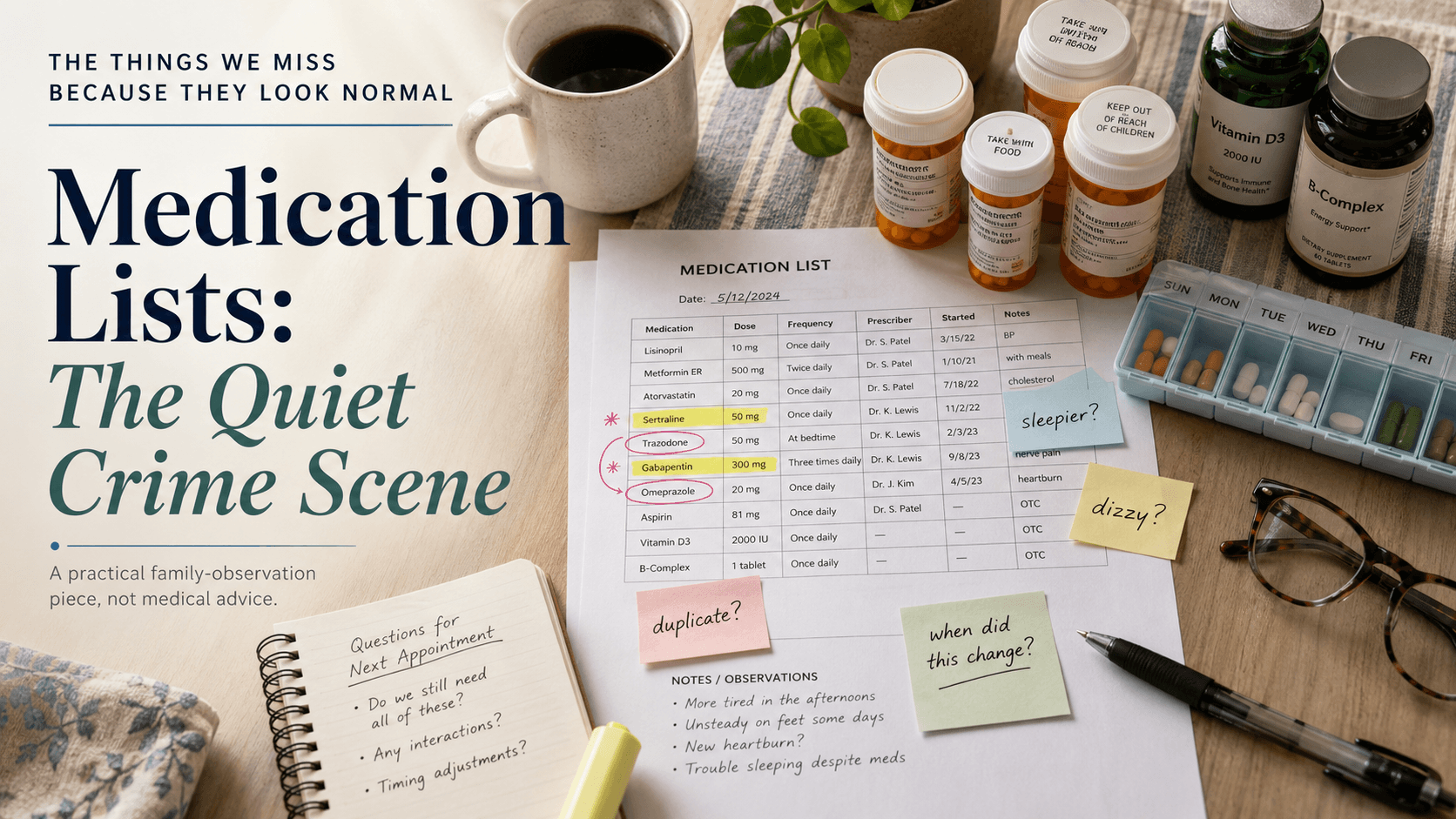
The Things We Miss Because They Look Normal
VS
Medication Lists: The Quiet Crime Scene
There is a particular kind of document that sits quietly in kitchens, purses, patient portals, discharge folders, and doctor’s offices.
It looks responsible.
It looks complete.
It looks like evidence that everyone knows what is going on.
The medication list.
And yet, sometimes, that tidy little list is not a list at all. It is a crime scene with excellent formatting.
Not because anyone is careless. Not because doctors are villains. Not because families are failing. But because medication lists can become one of those places where assumptions pile up, quietly and politely, like coats on a bed during a party.
One doctor adds something.
Another doctor changes something.
A hospital discharge note says one thing.
The pharmacy label says another.
A vitamin sneaks in through the side door wearing a “natural” hat.
An over-the-counter sleep aid arrives with the confidence of a tiny burglar.
And somewhere in all of this, the person at the center of the story begins acting differently.
More tired.
More confused.
More anxious.
More unsteady.
More flat.
More agitated.
Less themselves.
And because dementia is already in the room, everyone looks at the diagnosis first.
Of course they do.
The diagnosis becomes the loudest suspect.
But sometimes the diagnosis is not acting alone.
This is where families often notice what the system misses.
Not because families know more medicine. They usually do not. Not because they should be expected to become unpaid pharmacists at the kitchen table. That way lies madness, and possibly a three-ring binder with tabs.
Families notice because they live in the pattern.
They know what Tuesday morning usually looks like. They know whether Dad has always needed a nap after lunch or whether this is new. They know whether Mum has always been a little anxious before appointments or whether she is now pacing the hallway at 4 p.m. every day. They know when the person they love has gone subtly off-kilter.
That kind of noticing matters.
A medication list should not just answer, “What is being taken?”
It should help answer:
What changed?
When did it change?
Who changed it?
Why was it changed?
What happened afterward?
What else was added, stopped, doubled, missed, or misunderstood?
The quiet problem is that medication lists often freeze time. They capture a version of the truth, but not necessarily the living truth.
The list may say the medication is taken daily.
But is it?
The list may say the dose is 10 mg.
But is the bottle still 5 mg because the old refill is being used up first?
The list may say one medication was discontinued.
But is it still sitting in the weekly pill box because nobody knew it had been stopped?
The list may include prescriptions.
But does it include the antihistamine, the sleep aid, the pain reliever, the CBD gummy someone recommended, the magnesium powder, the “memory supplement,” the herbal tea, the old antibiotic in the bathroom cabinet, the occasional glass of wine, or the pill borrowed from a spouse because “it worked for them”?
This is not a lecture. It is a reality check.
Medication does not happen in a spreadsheet. It happens in a house.
It happens with refill delays, rushed appointments, tiny labels, different pharmacies, changing routines, and people trying very hard to stay independent.
For someone living with early cognitive change, the gap between the official medication list and the real-life medication routine can widen quietly. A pill taken twice because it was forgotten. A pill skipped because the morning got interrupted. A new side effect mistaken for decline. A decline assumed to be inevitable because the word Alzheimer’s has entered the room and started throwing its weight around.
That is the danger.
Once a diagnosis is attached to a person, normal questions sometimes stop being asked.
Is this confusion new?
Did it begin after a medication change?
Did sleep change first?
Did balance change first?
Did appetite shift?
Did agitation appear after the dose increased?
Did the “bad week” begin after the hospital visit?
Did anyone compare the bottles to the portal list?
Did anyone ask the pharmacist?
This is where MiM’s way of thinking becomes useful.
We are not trying to turn families into clinicians.
We are trying to preserve the everyday record.
Because the everyday record is often where the clues live.
A Supporter may not know whether a medication is causing a symptom. That is for a qualified medical professional to assess. But a Supporter can notice that the symptom began three days after a change. A Traveler may not remember whether they took the new pill at breakfast, but the household routine may show that the pillbox was opened twice. A family may not know what the answer is, but they can bring better questions.
And better questions can change the appointment.
Instead of saying, “He seems worse,” a family can say:
“He became much sleepier after the evening medication was added.”
“She started feeling dizzy the week after the dose changed.”
“He is more confused on the mornings after poor sleep.”
“She has been taking an over-the-counter sleep aid we did not realize mattered.”
“The pharmacy list, hospital discharge list, and pill bottles do not match.”
That is not medical advice.
That is evidence.
And evidence is precious.
The practical step is simple, though not always easy: build a living medication record.
Not just the name of each medication, but the real-world context around it.
Name. Dose. Time of day. Reason it was prescribed. Prescribing clinician. Pharmacy. Start date. Stop date. Dose changes. Side effects noticed. Supplements. Over-the-counter medications. Missed doses. Duplicate bottles. Old prescriptions still in circulation. Questions for the doctor or pharmacist.
Also note the human part.
Sleep. Appetite. Mood. Balance. Bathroom changes. Alertness. Agitation. Confusion. Falls. New fears. New routines. New resistance. New fatigue.
Not obsessively. Not with the joyless energy of a tax audit.
Just clearly enough that patterns have somewhere to land.
Because what looks like “just getting worse” may sometimes be something else.
Something adjustable.
Something explainable.
Something worth asking about before everyone surrenders to the diagnosis.
The medication list is not the enemy.
But an unexamined medication list can become a place where the story gets lazy.
And in early dementia, lazy stories are dangerous.
They flatten the person.
They make every change look inevitable.
They give the diagnosis too much power and the family too little information.
So no, families should not stop medications on their own. They should not play doctor. They should not go hunting through side-effect lists at midnight until the internet turns into a haunted forest.
But they can observe.
They can document.
They can compare.
They can ask.
They can bring the quiet crime scene into the light and say, kindly but firmly:
“Before we call this decline, can we please look at the whole list?”
That question may not solve everything.
But it can open a door.
And sometimes, in the long corridor after diagnosis, an open door is no small thing.